
An Algorithm for the Prevention and Treatment of Pain Complications of the Radial Forearm Free Flap Donor Site
Nicholas A Calotta, MD1, Akash Chandawarkar, MD2, Shaun Desai, MD1 and A. Lee Dellon, MD, PhD3, (1)Johns Hopkins University School of Medicine, Baltimore, MD, (2)Johns Hopkins School of Medicine, Baltimore, MD, (3)Plastic Surgery, Johns Hopkins University, Baltimore, MD
Introduction
The radial forearm free flap (RFFF) is a staple of microsurgical reconstruction. Significant attention has been paid to donor site morbidity, particularly vascular and aesthetic consequences. Relatively few authors have discussed peripheral nerve morbidity such as persistent hypoesthesia, hyperesthesia, or allodynia in the hand and wrist or neuroma formation in the wrist and forearm. Here we present a diagnostic and therapeutic algorithm for painful neurologic complications of the RFFF donor site.
Materials and Methods
The peripheral nerves that can be involved with the RFFF are reviewed with respect to the manner in which they may be involved in post-operative pain manifestations. The diagnostic role of nerve block is emphasized. A method for prevention and for treatment of each of these possibilities is also presented.
Results
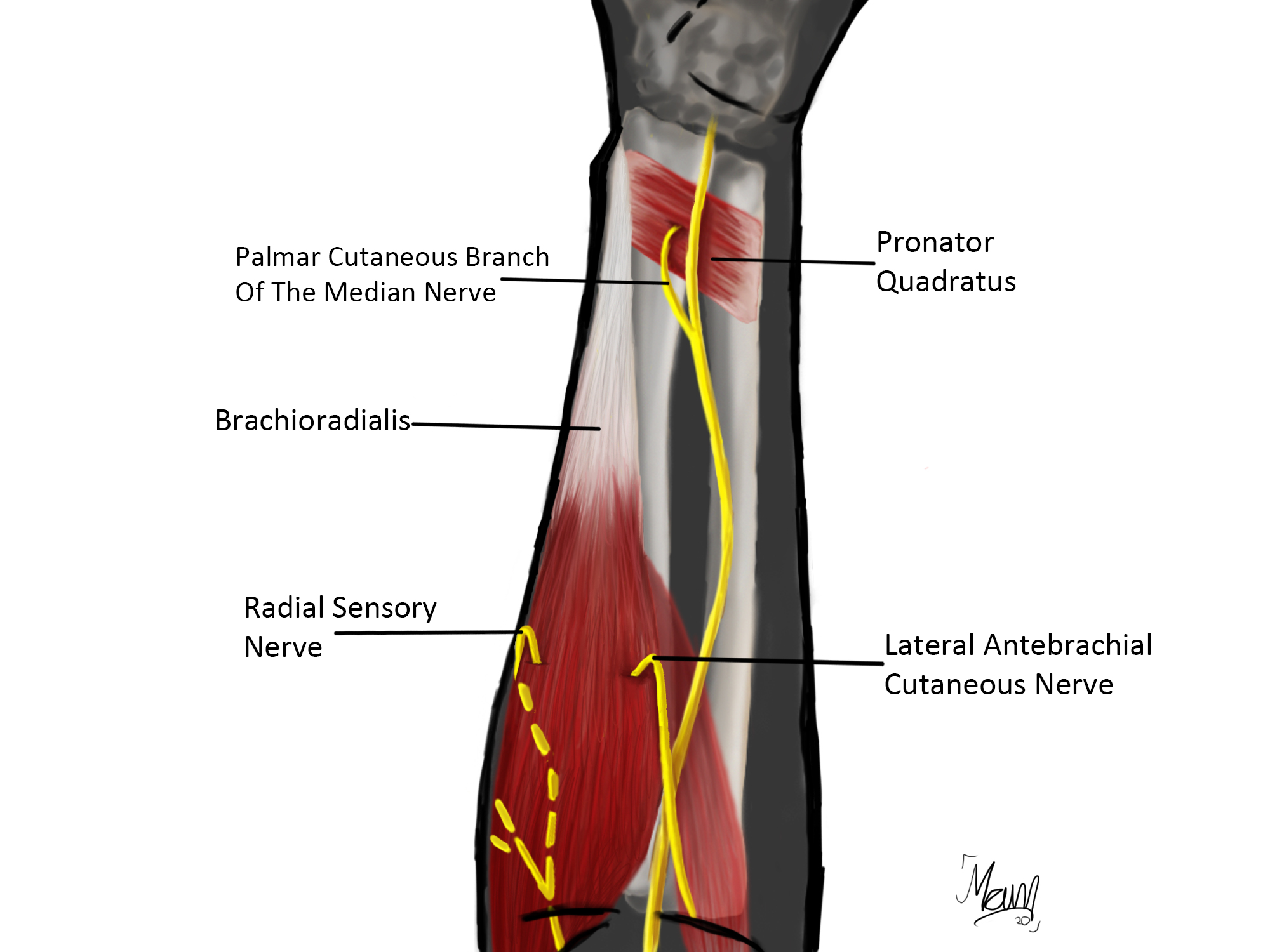
Nerves from the forearm that can be harvested with the RFFF will have the most likelihood for injury and these include the lateral antebrachial cutaneous nerve (LABCN), the radial sensory nerve (RSN), and the medial antebrachial cutaneous nerve (MABCN). A nerve that may be injured at the distal juncture of the skin graft to the forearm is the palmar cutaneous branch of the median nerve (PCBMN). The “prevention” portion of the algorithm suggests that each nerve divided to become a recipient nerve should have its proximal end implanted into a muscle to prevent painful neuroma. (Table 1) The “treatment” portion of the algorithm suggests that if a neuroma does form, it should be resected, not neurolysed, and the proximal portion be implanted into an adjacent muscle. (Table 2; Figure 1)
Conclusions
Neurological complications following RFFF can be prevented by an appropriate algorithm as described by devoting attention to the proximal end of recipient nerves. Neurological complications, once present, can be difficult to diagnose accurately. Nerve blocks are critical in this regard and are employed in the treatment algorithm presented.
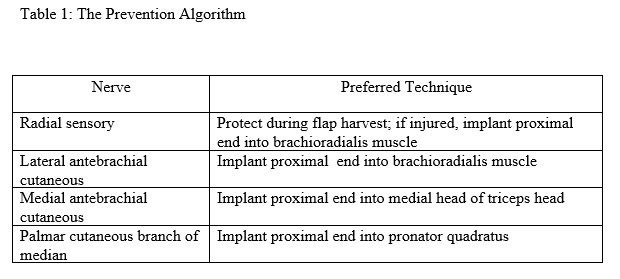
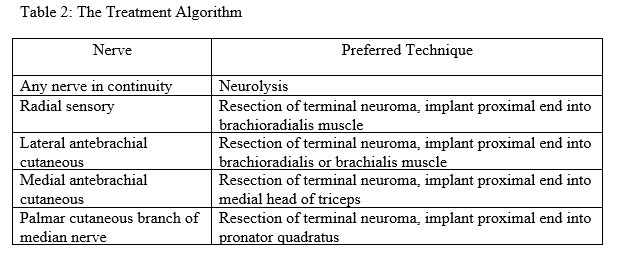
Figure 1: Nerve Implantation Schematic
Back to 2021 ePosters