
Diffusion MRI for Diagnosing Cubital Tunnel Syndrome: A Proof of Concept Study
Timothy Thomas Griffiths, MRES1, Irvin Teh, BE MBiomedE PhD1, Grainne Bourke, MB BCh BAO FRCSI FRCS(Plast)2, Ryckie George Wade, MBBS MSc MClinEd MRCS FHEA3 and Robert J Flather, MBChB1, (1)University of Leeds, Leeds, United Kingdom, (2)Leeds Teaching Hospitals Trust, Leeds, United Kingdom, (3)Department of Plastic and Reconstructive Surgery, University of Leeds, Leeds, United Kingdom
Introduction
Cubital tunnel syndrome (CuTS) affects 6% of the population causing pain, sensory disturbance and motor dysfunction. Postoperative complications include: failure to improve (30%), chronic pain (15-52%), infection (up to 7%), haematoma (3%), complex regional pain syndrome (1%) and recurrence (4%). Tests for CuTS lack reliability and diagnostic accuracy. Diffusion tensor magnetic resonance imaging (DTI) characterises tissue microstructure, providing indirect measures of nerve health which are sensitive to myelination, axon diameter, fibre density and organisation. DTI provides reliable objective data to provides insight into nerve function, beyond the capabilities of electrodiagnostics. DTI has not been tested in CuTS and represents the rationale for this study
Materials and Methods
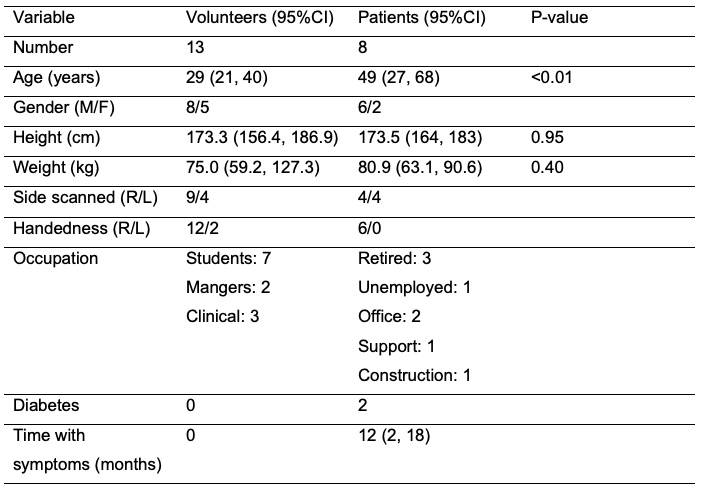
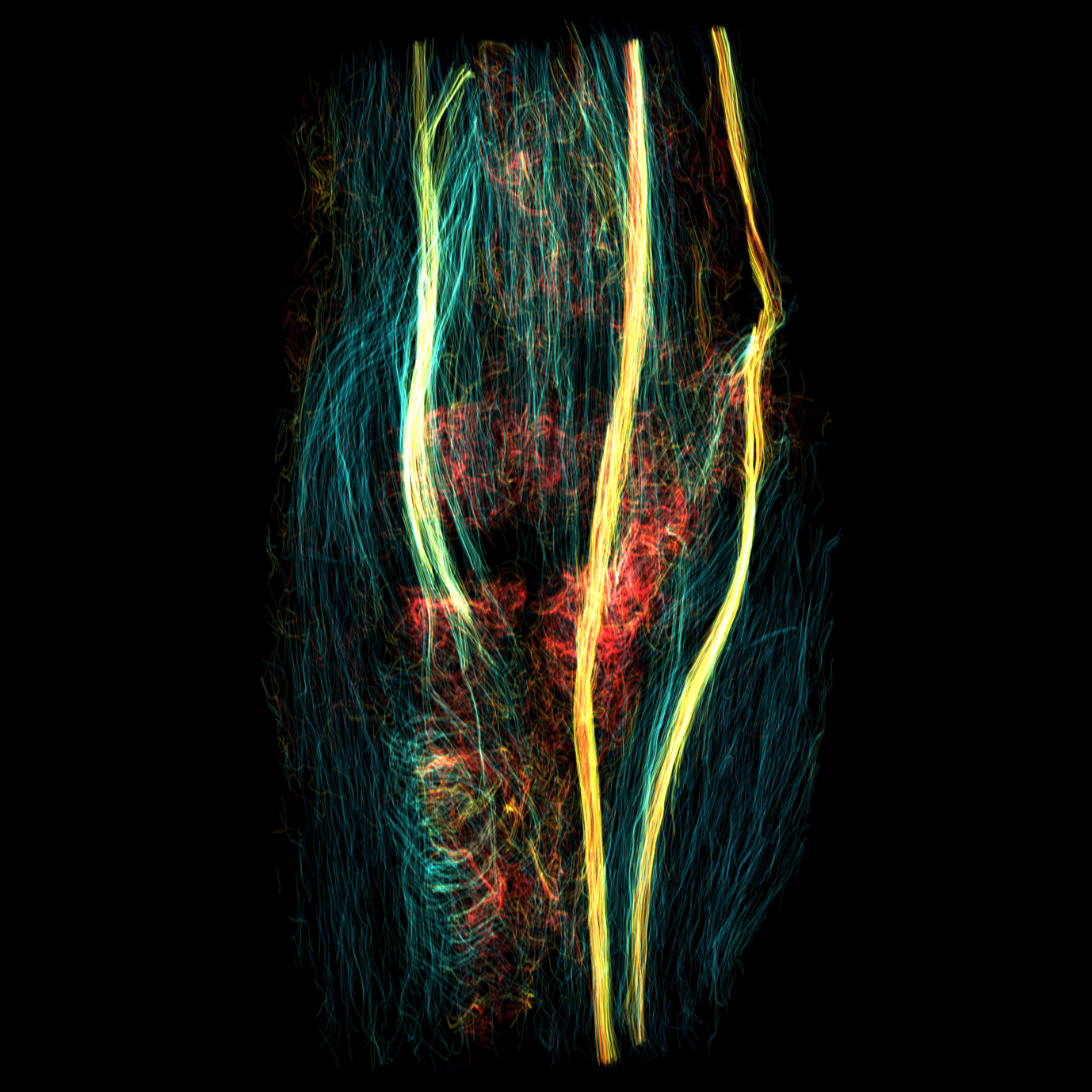
A prospective cohort study comparing DTI parameters in asymptomatic healthy volunteers and patients with CuTS awaiting surgery. DTI was acquired by single-shot echo-planar imaging using a Siemens Prisma (3 Tesla) as follows: TE 74ms, TR 7800ms, b-value 800 s/mm2, 3mm slice thickness with 1.5mm2 in-plane resolution, 30 diffusion directions with a dynamic excitation pulse. Data were reconstructed using generalised q-sampling in DSI Studio. Tensors were registered to T2-weighted images. Measurements were taken from the ulnar nerve at the anatomically defined midpoint of the cubital tunnel and compared using independent samples t-tests.
Results
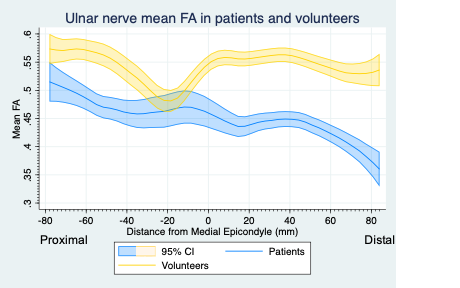
The ulnar nerve of patients with CuTS had a significantly lower fractional anisotropy (FA) (mean difference 0.15 [95% CI 0.07-0.23]) and higher radial diffusivity (mean difference 0.25 x10-3 mm2/s [95% CI (0.05-0.46) x10-3 mm2/s]). There were no significant differences in mean diffusivity, axial diffusivity or the normalised quantitative anisotropy. By linear regression FA inversely correlated with quickDASH scores and iHaND scores. DTI parameters monofilament or 2-point discrimination thresholds, or strength testing of the intrinsic muscles of the hand and grip strength.
Conclusion
Diffusion tensor imaging demonstrates differences in the fractional anisotropy and radial diffusivity of the ulnar nerve between healthy individuals and those with symptomatic cubital tunnel syndrome. This non-invasive scan could improve the diagnosis of cubital tunnel syndrome and thus benefit patients and clinicians alike.
Back to 2021 Abstracts