
Musculocutaneous Nerve Branches and Fascicles: A Cadaveric Study
Kevin T Rezzadeh, BA, New York University School of Medicine, New York, NY, Kameron Rezzadeh, MD, David Geffen UCLA Medical Center, Los Angeles, CA and Jacques Hacquebord, MD, NYU Langone Medical Center, New York, NY
Musculocutaneous Nerve Branches and Fascicles: A Cadaveric Study
Introduction:
The musculocutaneous nerve (MCN) is the recipient of nerve transfers for restoration of elbow flexion in patients with brachial plexus injury. Depending on feasibility and surgeon preference, either the MCN proper or the more distal motor branches will undergo neurotization with the nerve donor. The purpose of this study is to better delineate the relative branching pattern of the MCN and compare dimensions of MCN branches to the MCN proper.
Methods:
In this cadaveric study, the MCNs course was tracked and measured relative to distance from the acromion, normalized by humeral and arm length. Secondary outcomes included distance between the motor branch to the biceps (MBB) and motor branch to the brachialis (MBBr), lengths/cross-sections of the MCN proper and nerve branches along the MCN's course in the upper extremity, and relative position of nerve branches to the biceps. Nerve cross-sections were estimated using a caliper with a precision of ±0.03mm. Cross-sections of individual MCN branches were normalized by the cross-sectional area of the MCN proper.
Results:
The right arms of seventeen cadavers (11 males; 6 females) were used. The MBB was 12.6 cm (SD: 2.0 cm) from the acromion. This distance represented 40% the length of the humerus, and 17% of the length of the upper extremity. The MBBr was on average 18.6 cm (SD: 1.2) from the acromion. This distance represented 59% the length of the humerus, and 26% the length of the arm. The distance between the MBB and MBBr was 6 cm (SD: 1.2), which is 17.7% of the length of the humerus. In three cases, there were discrete branches to the common belly of the biceps. When divided by the area of the MCN, the MBB had 25% of this cross-sectional area, MBBr had 33% of this cross-sectional area. There were discrete fascicles to the biceps other than the MBB in 5 cases (30%).
Discussion:
In this study we describe the anatomy of the MCN in relation to the length of the upper extremity. Anatomical consistency between normalized distances will be useful in planning MCN neurotization and intraoperative identification of motor branches of the MCN. The greater variability in cross-sectional ratios of MCN branches along with the high incidence of fascicles to the biceps branching outside of the MBB are both very helpful in determining the optimal surgical plan.
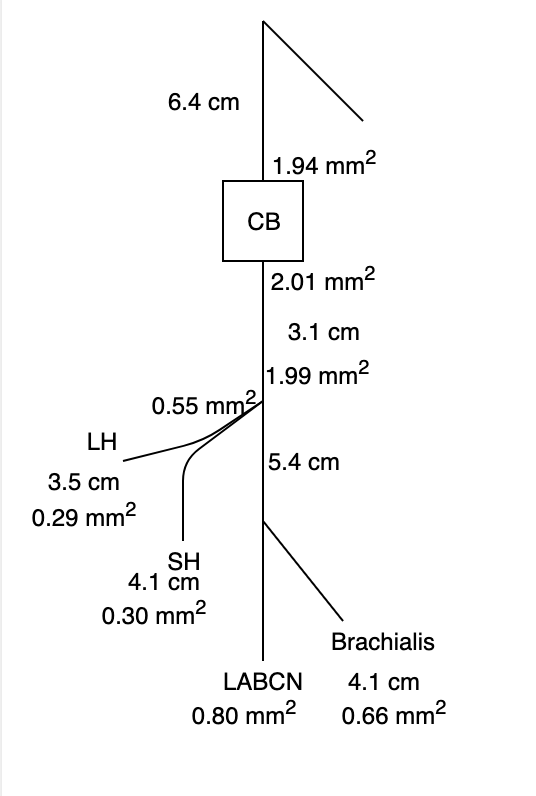
Figure 1:
Back to 2020 ePosters