
Direct Repair of Nerves Under Tension Has Better Functional and Histologic Outcomes Than Use of an Isograft
David M Brogan, MD, MSc1, Fraser J. Leversedge, MD2, Dana Rioux-Forker, MD3, Jason M Wever, MS4 and Christopher Dy, MD MPH FACS1, (1)Washington University School of Medicine, St. Louis, MO, (2)Department of Orthopaedic Surgery, DUKE UNIVERSITY, Durham, NC, (3)University of Missouri, Columbia, MO, (4)Washington University in St. Louis, St. Louis, MO
Abstract
Purpose: The ideal method of repairing a nerve with a small segmental defect is unknown. Potential options include mobilization and primary repair under tension, splinting of the nerve with a conduit, or repair with an interpositional isograft. We investigated the effect of each of these repair techniques on functional and histological outcomes in a rat segmental nerve defect model.
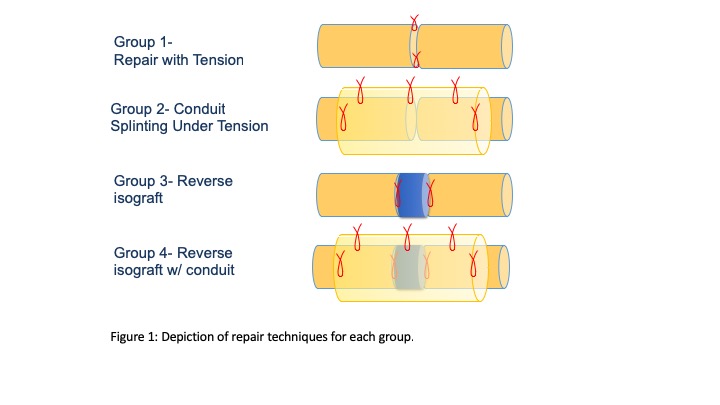
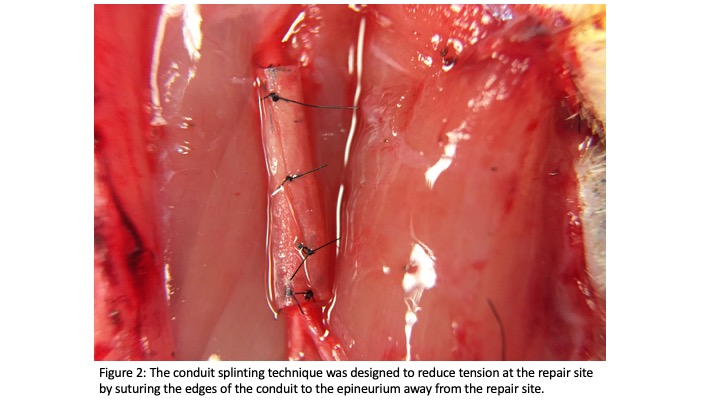
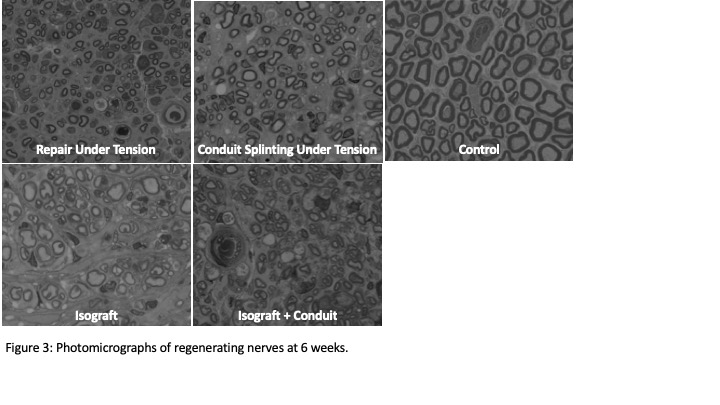
Methods: Forty Lewis rats were divided into 4 groups of 10, with a different repair technique performed in each group. A unilateral sciatic nerve segmental defect was created in each rat by excising 5 mm of sciatic nerve in a standardized fashion. The segmental defect was then repaired or reconstructed using one of four techniques: primary repair under tension, repair with use of a conduit splint, reverse isograft with conduit splinting, and reverse isograft without splinting (Figures 1 & 2). After 6 weeks, functional outcomes were assessed by measuring Sciatic Functional Index (SFI) using walking track analysis. Histologic outcomes were also assessed using a semi-automated detection algorithm to measure number of axons, axonal size, density, amount of debris and remyelination (Figure 3). Normality of the data was assessed with Shapiro-Wilks test. Kruskal-Wallis test with adjustment for normal comparisons was utilized to compare histologic parameters among groups.
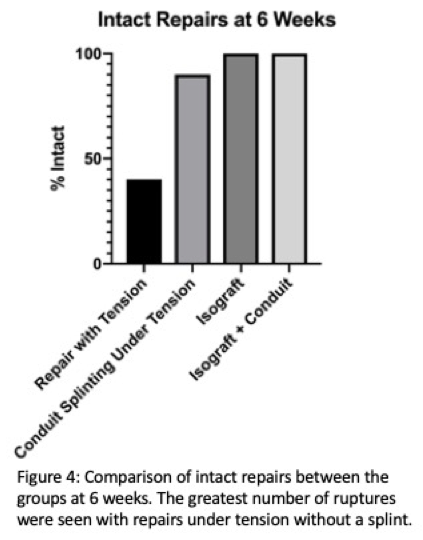
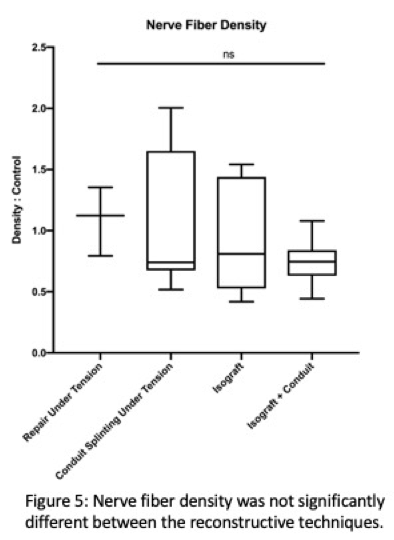
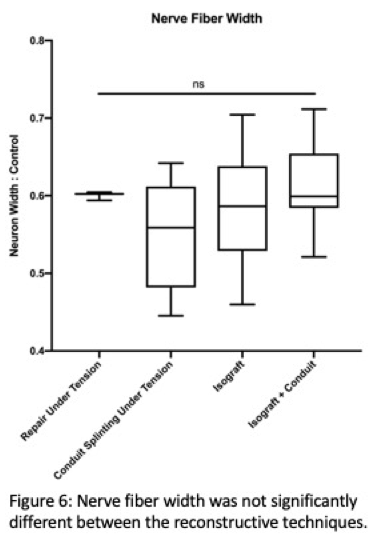
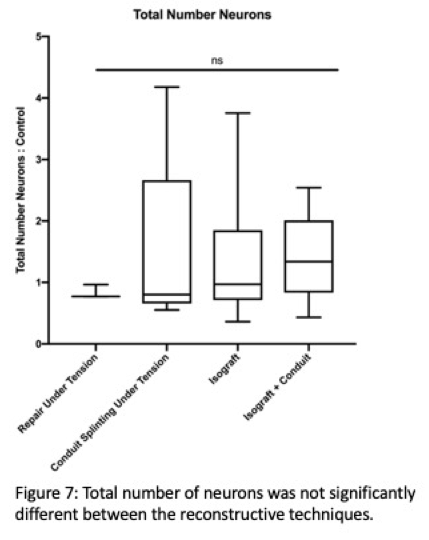
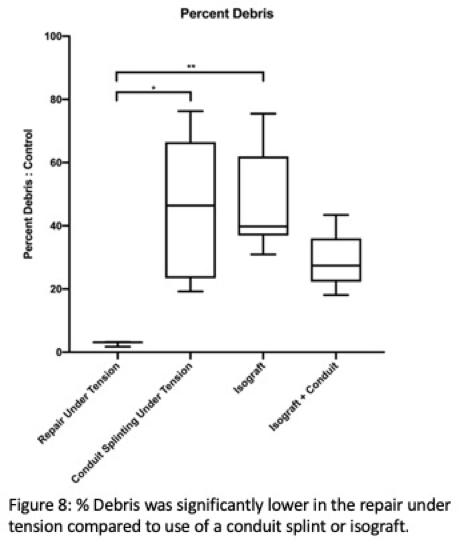
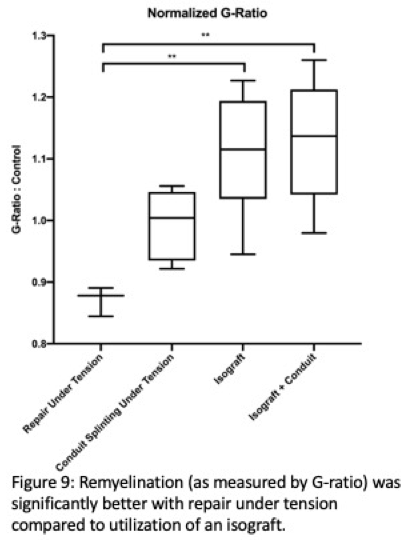
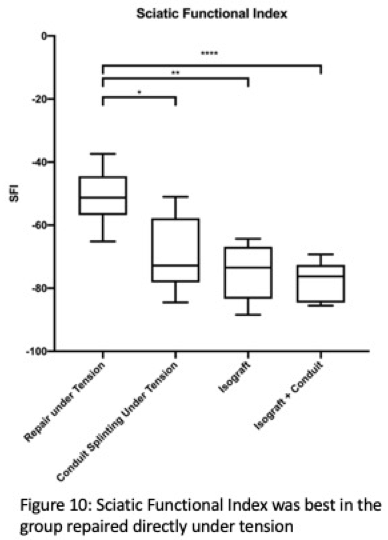
Results: Nerve splinting with a conduit reduced repair site rupture rates compared to a conduit alone (Figure 4). For repairs under high tension, conduit splinting resulted in similar axon density (Figure 5), size (Figure 6) and number (Figure 7). More debris was found with use of a conduit splint or isograft alone compared to primary repair under tension (Figure 8) and remyelination, as measured by G-ratio, was better with primary repair under tension compared to use of an isograft (with or without conduit) (Figure 9). The best functional outcomes, as measured by SFI, were found in primary repairs under tension (Figure 10).
Conclusions: Mitigating tension at the coaptation site through a technique of nerve conduit splinting had a trend towards reduced rupture rates for nerve repairs associated with a segmental defect. Of interest, outcomes of primary nerve repair under tension that did not rupture demonstrated better functional results at 6 weeks compared to splinting or reverse isograft groups. While repair under tension has the potential to lead to catastrophic failure, those that remain intact may perform better than defects reconstructed with an isograft.
Level of Evidence: Level I
Back to 2020 ePosters