
Endoscopic Nerve Decompression In The Lower Extremity: Limiting Incisional Morbidity
Chris Devulapalli, MD; Kenneth Fan, MD; Grant M Kleiber, MD
Georgetown University Hospital, Washington, DC
Introduction
Open approaches to decompression of the tibial nerve at the tarsal tunnel and superficial peroneal nerve (SPN) in the lateral leg compartment have proven beneficial in patients with compression and/or diabetic neuropathy. The merit in such procedures, however, may be overturned by prolonged immobilization and high rates of wound dehiscence, particularly in the diabetic population. We propose a novel endoscopic technique for nerve decompression of the tibial nerve and its branches through the medial ankle, as well as the SPN through the lateral leg compartment.
Methods:
All procedures were performed using an endoscopic retractor fitted with a 4 mm endoscope under tourniquet control on an outpatient basis. Patients were evaluated for signs of tibial neuropathy at the medial ankle, and/or SPN neuropathy based on location of presenting neuropathic symptoms and examination of TinelŐs signs. Decompression of the tibial, medial/lateral plantar, and medial calcaneal nerves were performed through a 2 cm transverse incision posterior to medial malleolus. SPN decompression was performed through a 3 cm incision made 15 cm proximal to the lateral malleolus and 4 cm lateral to the tibial crest, decompressing the nerve through its subfascial course until its exit from the transverse crural ligament. All patients were immediately mobilized with full weight-bearing status. Patients were followed postoperatively to assess for improvement in symptoms.
Results:
Endoscopic neuroplasty was performed on 7 lower extremities, with decompression of the tarsal tunnel and/or SPN (4 underwent both, 2 underwent SPN release only, and 1 underwent tarsal tunnel release only). Patients ranged from 42-63 years, BMI ranged from 20.6 to 38.7 kg/m2, and two patients had diabetes. All patients had successful endoscopic release without any intraoperative complications, nerve/vessel injuries, or conversion to open approach. Within a 2-7 month follow-up, all patients reported significant improvement in pain and sensation in the affected nerve distribution. All incisions completely healed without any wound healing complications.
Discussion:
We present a novel endoscopic approach for complete tarsal tunnel and superficial peroneal decompression. These procedures can be performed both safely and effectively to relieve lower extremity compression neuropathies while limiting potential incisional morbidity, particularly in high-risk diabetic patients.
Figure 1. Endoscopic view of medial and lateral plantar nerves, fully decompressed through tarsal tunnel.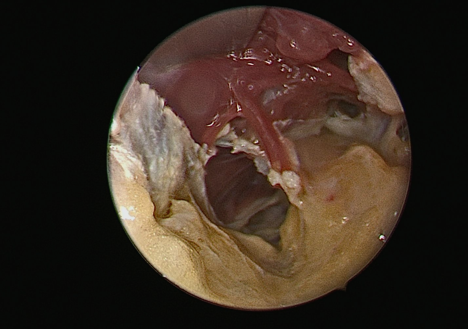
Figure 2. Incision for endoscopic tarsal tunnel decompression. Dotted lines demonstrate open approach.
Back to 2019 Abstracts