
Regenerative Agonist-Antagonist Myoneural Interface for Neural Prosthetic Control
Shriya S Srinivasan, BS1,2; Matthew J. Carty, MD3; Peter Calvaresi, n/a1; Anthony Zorzos, PhD1; Tyler Clites, BS1; Hugh Herr, PhD1; Benjamin Maimon, B.S.4; Cameron Taylor, BS, MS4; (1)Massachusetts Institute of Technology, Cambridge, MA, (2)Harvard Medical School, Boston, MA, (3)Division of Plastic Surgery, Brigham and Women's Hospital, Boston, MA, (4)MIT, Cambridge, MA
Introduction: During a standard amputation, nerves are transected, causing painful neuromas and rendering efferent recordings infeasible for robust prosthetic control. Furthermore, physiological agonist-antagonist muscle relationships are severed, precluding the generation of musculotendinous proprioceptive afferent signals. This afferent feedback is critical for joint stability, trajectory planning, and fine motor control. Here, we created and evaluated an Agonist-antagonist Myoneural Interface (AMI), a novel surgical paradigm for peripheral nerve interfacing, which reinstates the antagonist-agonist architecture native to intact musculoskeletal anatomy and provides a robust method for efferent and afferent signaling with motor nerves.
Materials & Methods: Tendons from two deinnervated, devascularized muscle grafts were surgically coapted to form an agonist-antagonist pair and secured to fascia in 7 murine subjects. Each graft was neurotized with either the peroneal or tibial nerve. After 4 months, we electrically stimulated the regenerated motor nerve of the agonist muscle while measuring the strains in each muscle, agonist EMG and the afferent ENG signal generated by the antagonist muscle. To isolate the dependence of afferent feedback on an agonist-antagonist structure, the linked muscles were separated. ENG and EMG signals from both muscles were measured in response to electrical stimulation. Finally, we performed histology of the harvested AMI to assess healing and regeneration.
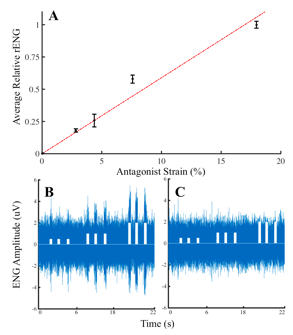
Results: Monthly insertional EMG testing revealed reinnervation levels comparable to healthy muscles at 3-4 months after surgery. EMG from the agonist muscle proportionally scaled with stimulation amplitude (average r2 = 0.85 for n=7) and yielded a proportional stretch in the antagonist muscle (range of strain: 0.08 +/- 0.03 to 0.23 +/- 0.14), but no co-contraction or EMG spikes. Furthermore, afferent signals were generated from the antagonist muscle and linearly correlated to the strains generated (r2= 0.96) (Fig 1 A, B). Once the agonist-antagonist link was severed, no afferent signals were generated (Fig 1C). Histology indicated regenerating myocytes, healthy neural tissue and viable muscle spindle fibers, primarily responsible for generating afferent signals in response to stretch.
Conclusions: In this study, validation of the AMI model resulted in graded efferent EMG and afferent ENG signals generated from functionally regenerated myoneural constructs. The AMI framework has the potential to enable robust peripheral nerve interfacing capable of natural efferent and afferent signaling in human subjects.
Fig 1. (Stimulation pulses (white) = 0.5, 1, 2 mA)
Back to 2018 Program