
Outcomes and Cost Analysis of Needle Aponeurotomy, Collagenase Injection, and Fasciectomy in the Treatment of Dupuytren's Contracture
Nels Leafblad, MD; Eric Wagner, MD; Nathan R Wanderman, MD; Marco Rizzo, MD; Sue Visscher, PhD
Mayo Clinic, Rochester, MN
Purpose:
The aim of our study was to evaluate demographics, repeat interventions and their associated risk factors, and cost of three common treatments for Dupuytren's contractures, including needle aponeurotomy (NA), collagenase injection, and open fasciectomy.
Methods:
We performed a retrospective review examining a consecutive series of 859 fingers with Dupuytren's contractures treated by a single surgeon from 2005 to 2016 at our institution, including needle aponeurotomy (NA) (n=450), collagenase injection (n=274), and fasciectomy (n=135). We collected basic demographics, presenting contractures, and co-morbidities. Outcomes analyzed included need for repeat intervention overall and multiple (greater than 1) repeat interventions. The average standardized direct medical costs in 2016 inflation-adjusted dollars of the initial treatment episodes were calculated for the three groups.
Results:
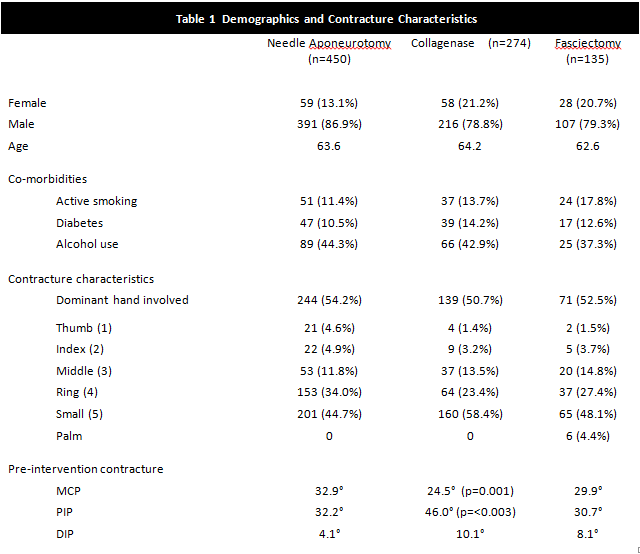
Demographics were similar between the three treatment groups (Table 1). The fifth finger was the most commonly affected digit including 45% of the NA, 58% of collagenase, and 48% of the fasciectomy groups. Collagenase had the lowest pre-intervention MCP contracture at 24.5° compared to 33° in the NA group, and 30° for the fasciectomy group (p=0.001), while collagenase had the highest PIP and DIP contractures (46° and 10°), compared to NA (32° and 4°), and fasciectomy (31° and 8°), (p=<0.003).
Collagenase had the highest rate of repeat interventions (37%) compared to NA (26%), and fasciectomy (6%), (p=<0.001). Collagenase also had a higher percentage of fingers needing 2 or more interventions (13%), compared to NA (6%) and fasciectomy (2%), (p=<0.001). In the NA group, the factors leading to repeat interventions included younger age (p=0.03), larger PIP contracture (p=0.02), larger DIP contracture (p=0.047), and use of blood thinners (p=0.049); in the collagenase group younger age (p=0.01) and larger PIP contracture (p=0.001); and there were no significant factors leading to repeat intervention in the fasciectomy group. The standardized costs for initial treatment of a single finger by NA, collagenase, and fasciectomy were $825, $4,008, and $4,812, respectively. Including all repeat interventions, the cumulative costs of NA, collagenase, and surgery were $1,694, $5,903, and $5,157, respectively (Table 2).
Conclusions:
Treatment with collagenase resulted in the highest rate of repeat interventions as well as the highest cumulative cost over time. Larger contractures at the PIP joints and younger age at time of initial intervention correlate with both increased rates of repeat interventions as well as cumulative cost in the collagenase and NA groups. Though fasciectomy had the highest initial cost, the costs thereafter were significantly less.
Back to 2018 ePosters