
Back to 2017 Annual Meeting Program
Reliability of Various Predictors for Preoperatively Accurate Diagnosis of Infraclavicular (Level IV) Adult Brachial Plexus Injury When Combined Paralysis of Shoulder and Elbow Encountered
Johnny Chuieng - Yi Lu, MD1; Tommy Nai-Jen Chang, MD1; Shan Shan Qiu, MD2; David Chwei-Chin Chuang, MD1
1Chang Gung Memorial Hospital, Chang Gung Medical College and Chang Gung University, Taoyuan, Taiwan, 2Maastricht University Medical Center, Maastricht., Netherlands
Introduction: Patients presenting with elbow and shoulder paralysis but are misdiagnosed preoperatively as supraclavicular or infraclavicular BPI are rare but can occur (Figure 1). In order to avoid big incision (from upper medial arm to neck) and unnecessary dissections by accurately diagnosing the correct level of injury, our goal was to evaluate the reliability of various predictors including trauma history, clinical motor and sensory examination, tinel sign, electrodiagnosis and radiologic studies.
Material and method: A retrospective study of 75 brachial plexus injuries from 2004 to 2013 with shoulder and elbow paralysis was performed. Clinical symptoms and signs neurological motor and sensory examinations, electrodiagnosis with EMG and NCV, radiology examination (plain X-ray, and/or imaging studies) which were routinely performed were recorded. A preoperative diagnosis was made first. The patients underwent surgical exploration and any discrepancies between preoperative and intraoperative findings were recorded. The reliability of different preoperative predictors were made for their accuracy in predicting the level of injury.
Results: 46 of those patients presented supraclavicular BPI, while 29 patients were diagnosed with infraclavicular BPI. In terms of history taking and preoperative examination, infraclavicular tinel sign was the most accurate predictor (OR 11.738), with scapular fracture being the next most reliable. With the assistance of EMG/NCV, an innervated clavicular head of pectoralis major (OR36.562) , biceps, teres major, serratus anterior and latissimus dorsi muscles would significantly differentiate level IV infraclavicular BPI from supraclavicular BPI (Figure 2 to 4).
Conclusion: This study has proven that certain pre-operative predictors are more reliable in differentiating diagnosis of level IV from level I to level III BPI.
Figure 01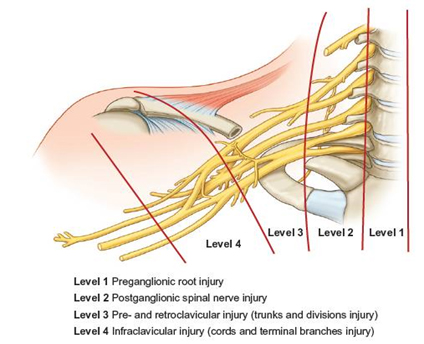
Figure 02 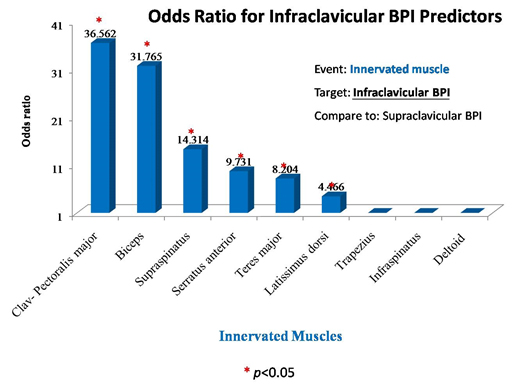
Figure 3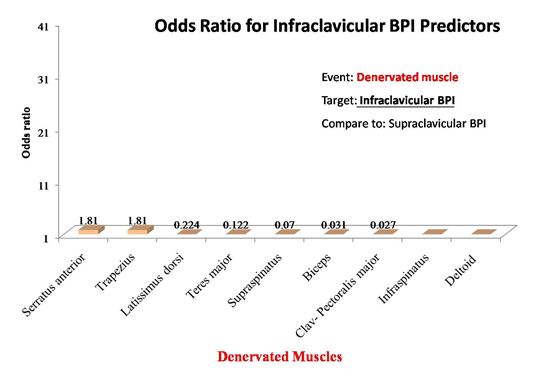
Figure 4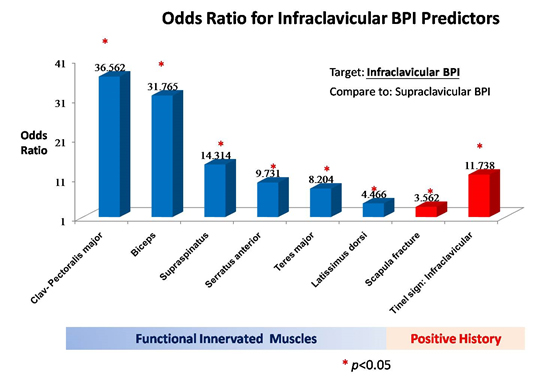
Back to 2017 Annual Meeting Program