
Back to 2015 Annual Meeting Program
Obstetrical Brachial Plexus Palsy: Can Excision of Upper Trunk Neuroma and Nerve Grafting Improve Function in Babies with Adequate Elbow Flexion at Nine Months of Age?
Lorelei Grunwaldt, MD1; Jack E. Brooker, MChem, MD2; Megan Natali, MD1; Megan Stranger, MD1
1University of Pittsburgh, Pittsburgh, PA; 2School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom
Introduction: Accepted indications for exploration in obstetrical brachial plexus palsy (OBPP) vary by center. Most agree that full elbow flexion against gravity at 9 months of age excludes a baby from surgical intervention. In infancy there are certain movements that are difficult to assess and less common for a baby to use such as shoulder external rotation and forearm supination. However the latter are extremely important for normal function as they grow.
Methods: A retrospective review of all obstetrical brachial plexus patients treated at a major multidisciplinary children's center was performed from 2009 to 2014. All patients were evaluated by a single PT and a single surgeon and the Toronto Active Movement Score (AMS) system was used. Those patients who had operative intervention were selected out for further review. Further analysis identified a cohort with isolated upper trunk lesions who had an active movement scale score of 5 or better for elbow flexion. Data analysis was performed on this group to look for improvement in overall function.
Results: 23 underwent operative intervention. 5 out of the 23 (22%) had isolated upper trunk lesions and elbow flexion AMS scores of 5/7 or better at the time of exploration. All 5 had weakness in shoulder abduction, flexion, external rotation as well as forearm supination. The average age at operative intervention was 10.8 months. Average follow-up was 22 months. All 5 had excision of neuroma between c5 and c6 and the upper trunk. Reconstructions were with sural nerve graft to either the anterior and posterior divisions of the upper trunk or, alternatively, the upper trunk proximal to the takeoff of the suprascapular nerve. In the case of the former a spinal accessory to suprascapular transfer was also performed. All patients except one, who was 4 months postop at time of evaluation, either returned to or exceeded their preoperative scores in the above mentioned shoulder and forearm movements. Their elbow function was preserved or improved (Table 1).
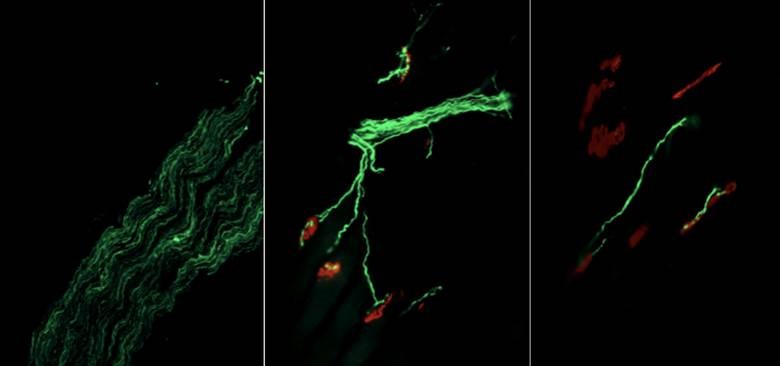
Figure 1: Neuromuscular junction staining of soleus muscle in GH-treated animals (left, middle) and control (right).
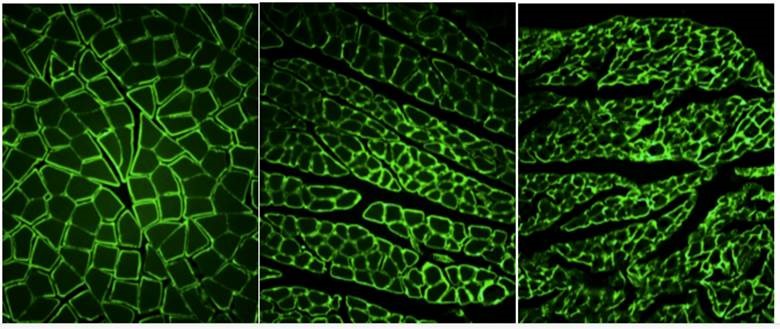
Figure 2: Laminin staining of cross-sections of non-denervated (left), GH-treated (middle), and untreated (right) gastrocnemius muscle.
Conclusion: In select cases of isolated upper trunk OBPP, operative intervention despite adequate elbow function can improve overall patient shoulder and forearm functional movement. There is no evidence that excision of neuroma with nerve grafting causes loss of elbow function or worsening of overall outcome.
Back to 2015 Annual Meeting Program