
Back to 2014 Annual Meeting Program
Real-time Control of a Prosthetic Hand with a Regenerative Peripheral Nerve Interface
Christopher M. Frost, BSE1, Andrej Nedic, MSE1, Daniel Ursu, MS2, Jana D. Moon, BS3, Brent Gillespie, PhD2, Nicholas B. Langhals, PhD1, Paul S. Cederna, MD3 and Melanie G. Urbanchek, PhD1
1Section of Plastic and Reconstructive Surgery, University of Michigan, Ann Arbor, MI, 2Mechanical Engineering, University of Michigan, Ann Arbor, MI, 3Department of Surgery, Section of Plastic Surgery, University of Michigan, Ann Arbor, MI
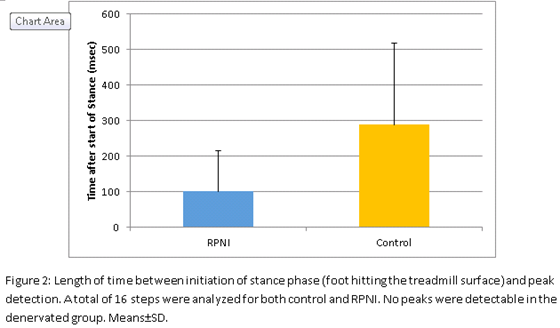
Introduction: Regenerative peripheral nerve interfaces (RPNI) are devices for signal transfer between peripheral nerves and amputee prosthetics. RPNI devices in rats have shown long term viability of 2 years. Still, signal and control algorithms for translating EMG signals in the interface into real-time control of a neuroprosthesis have not been established. Our purpose was to design a system for validating translation of EMG signals from an RPNI device into direct control of a neuroprosthetic hand. Methods: Three surgical groups were created in a rat model: control (n=3), denervated (n=3) and RPNI (n=3). For the RPNI group, a free soleus muscle transfer to the lateral thigh was performed. The transferred muscle was additionally reinnervated with the tibial nerve. For the denervated group, the tibial nerve was removed. In all groups, bipoloar electrodes were placed on the soleus muscle. Rats walked on a treadmill while EMG data were recorded 100 days after surgery. An EMG signal processing system was designed using LabVIEW. Raw EMG signals were processed. Using EMG peak detection, an activation sine wave was output to control a commercial myoelectric hand (DMC+ OttoBock) (Fig 1). The system was validated by comparing prosthesis activation to rat stance during EMG recording. Results: Preliminary data validates the EMG processing system. The total number of peaks detected in the control and RPNI groups closely matched the number of steps taken with an error rate of 1.02±7.67% and 3.9±6.7%, respectively. A total of 414 RPNI, 518 control and 225 denervated steps were analyzed. A subset of 16 gait cycles in each group were further examined to determine where peak detection occurred in the cycle. As expected peak detection in both control and RPNI groups occurred after the initiation of stance phase. On average peaks were detected 289±229 msec after initiation of stance phase in the control group and 100.1±115.3 msec in the RPNI group (Fig 2). Stance phase averaged 323.4±69.1 msec for Control and 316.7±78.4 msec for RPNI. As expected, no activation occurred for the denervated group. Conclusion: We demonstrated that RPNI signals can accurately control a prosthetic limb. 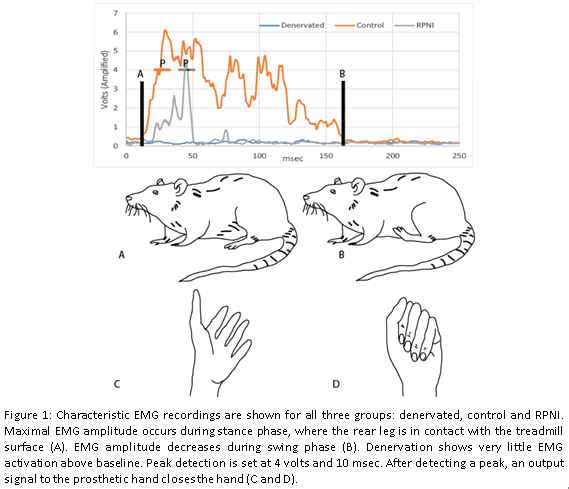
Back to 2014 Annual Meeting Program